
Epigastric vs. Abdominal Pain Symptom Checker
Assess Your Pain
Results & Recommendations
Select your symptoms and click "Analyze Symptoms" to see the assessment.
Key Takeaways
- Epigastric pain sits in the upper middle abdomen, while abdominal pain can originate anywhere below the ribs.
- Common triggers for epigastric pain include gastric ulcer, GERD, gallstones and pancreatitis.
- Lower abdominal pain often points to IBS, appendicitis or colonic issues.
- Character of the ache (burning vs cramping), timing with meals, and associated symptoms help separate the two.
- Seek urgent care if pain is severe, sudden, or accompanied by fever, vomiting, or chest discomfort.
When a discomfort shows up just under the breastbone, many people wonder whether it’s a stomach issue or something more serious. The answer often lies in where the pain is felt and what else is happening in the body. This guide walks you through the anatomy, the usual suspects, and the red‑flag signs so you can tell the difference between epigastric pain and general abdominal pain.
What Exactly Is Epigastric Pain?
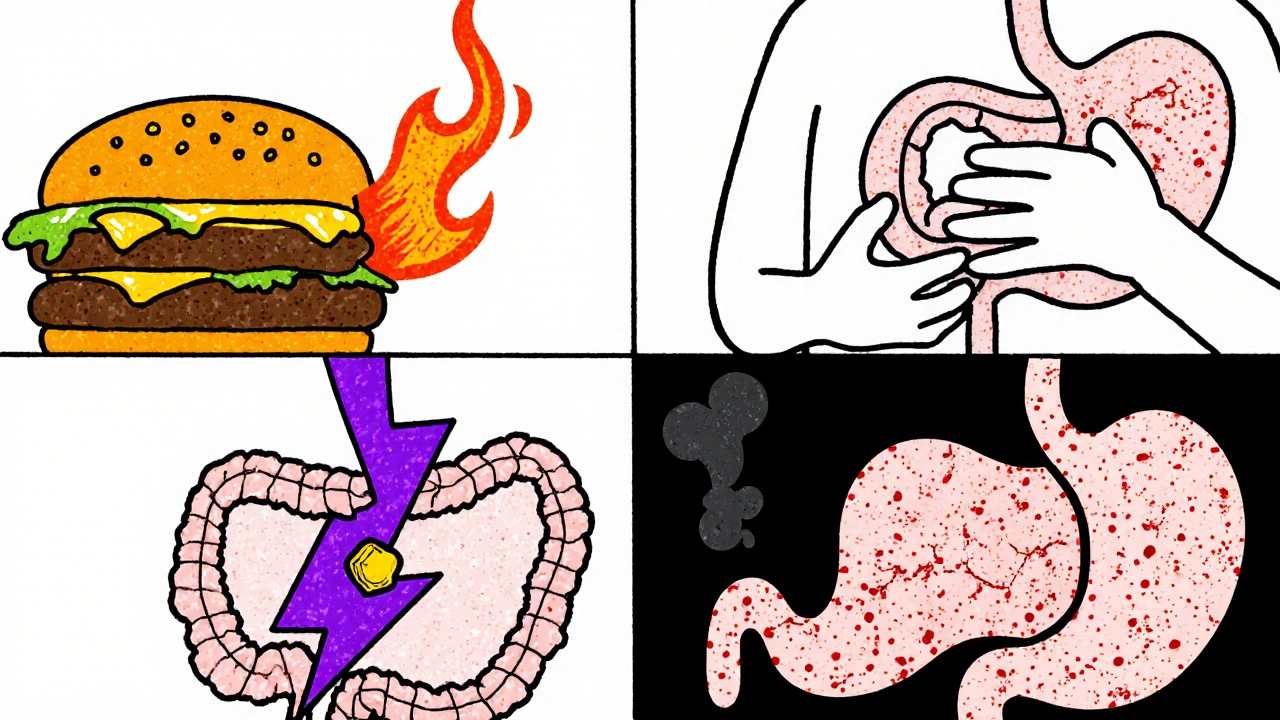
Epigastric Pain is a sharp or burning sensation localized in the upper central region of the abdomen, just below the sternum and above the navel. It often radiates upward toward the chest or downward toward the back. This area, called the epigastrium, houses the lower part of the esophagus, the stomach, the liver, the gallbladder, and the head of the pancreas.
What Is Abdominal Pain?
Abdominal Pain refers to any discomfort that occurs anywhere within the belly, from just below the ribs down to the pelvic floor. Because the abdomen contains a long chain of organs, the pain can be localized, diffuse, or refer to other body parts.
Why the Confusion?
Both pain types can feel similar-burning, cramping, or gnawing-and they often overlap with chest discomfort. The key to untangling them is to map the pain’s location, onset, triggers, and accompanying signs.
Quick Anatomy Overview
Understanding which organ sits where helps you match symptoms to structures. Below is a simplified map:
- Epigastrium (upper middle abdomen): Stomach, duodenum, head of pancreas, liver’s left lobe, gallbladder.
- Right upper quadrant: Liver, gallbladder, right kidney.
- Left upper quadrant: Spleen, stomach, distal pancreas.
- Lower abdomen (pelvic region): Small intestine, large intestine, appendix, reproductive organs.
Common Causes of Epigastric Pain
Here are the top culprits that usually sit in the epigastric zone:
- Gastric ulcer, also known as a peptic ulcer, creates a burning pain that often improves after eating or with antacids.
- Gastroesophageal reflux disease (GERD) or simple heart‑burn, causes a sour taste and pain that worsens when lying down.
- Gallstones may block the cystic duct, leading to a steady ache that spikes after fatty meals.
- Pancreatitis produces a deep, radiating pain to the back, often accompanied by nausea.
- Heartburn (a milder form of GERD) can mimic epigastric pain but is usually relieved by upright posture.
Common Causes of General Abdominal Pain
When the discomfort spreads lower or is diffuse, the following conditions are typical:
- Irritable bowel syndrome (IBS) causes cramping that improves after a bowel movement and is linked to stress.
- Appendicitis starts near the belly button and moves to the lower right quadrant, often with fever.
- Diverticulitis (outpouchings in the colon) leads to left‑lower‑quadrant pain and possible constipation.
- Gynecological issues such as ovarian cysts or endometriosis, produce pelvic pain that may be cyclic.
- Urinary tract infection (UTI) can cause suprapubic discomfort and a burning sensation during urination.
Spotting the Differences - A Symptom Checklist
Use this quick‑scan list to see where your pain fits:
| Feature | Epigastric Pain | General Abdominal Pain |
|---|---|---|
| Typical Location | Upper middle abdomen, just below sternum | Anywhere below rib cage; often lower quadrants |
| Common Triggers | Meals (especially fatty), lying down, alcohol, NSAIDs | Stress, irregular bowel habits, infection |
| Radiation | Often to back or chest | May radiate to groin or thigh |
| Associated Symptoms | Heartburn, nausea, belching, early satiety | Diarrhea, constipation, fever, urinary symptoms |
| Pain Quality | Burning, gnawing, pressure | Cramping, sharp, colicky |
| Response to Antacids | Often improves | Usually no effect |

Red‑Flag Signs - When to Call a Doctor
Both pain types can signal something serious. Seek urgent medical attention if you notice:
- Sudden, severe pain that peaks within minutes.
- Pain accompanied by fever > 38°C (100.4°F) or chills.
- Persistent vomiting, especially if you can’t keep fluids down.
- Blood in vomit or stool, or black‑tarry stools.
- Difficulty breathing, chest tightness, or pain that spreads to the jaw/left arm (rule out cardiac causes).
- Unexplained weight loss or loss of appetite over weeks.
Diagnostic Tools Doctors Use
Based on your symptom pattern, a clinician may order one or more of the following:
- Physical exam: Tenderness points, rebound, guarding.
- Blood tests: CBC, liver enzymes, pancreatic enzymes (amylase/lipase), H. pylori antibody.
- Imaging: Ultrasound for gallstones, CT scan for pancreas or appendix, upper GI series for ulcers.
- Endoscopy: Direct look at esophagus, stomach, duodenum for GERD or ulcers.
- Stool studies: Check for infection, occult blood.
Self‑Care Tips While You Wait for an Appointment
If your pain isn’t an emergency, try these measures:
- Keep a food and symptom diary for at least three days.
- Avoid trigger foods: caffeine, alcohol, spicy or fatty meals.
- Take an over‑the‑counter antacid (e.g., calcium carbonate) for burning epigastric pain.
- Eat smaller, more frequent meals and stay upright for 2‑3 hours after eating.
- Practice stress‑reduction techniques (deep breathing, light walking) if IBS is suspected.
- Hydrate well, but limit carbonated drinks that can increase bloating.
Bottom Line
Distinguishing epigastric pain from broader abdominal pain hinges on location, timing, radiation, and accompanying signs. Knowing the likely culprits-like gastric ulcer or gallstones for upper‑midline pain and IBS or appendicitis for lower‑quadrant discomfort-helps you decide whether home care is enough or a medical visit is urgent.
Is epigastric pain the same as heartburn?
They feel similar, but heartburn is specifically acid reflux that rises into the esophagus, while epigastric pain can stem from a broader range of stomach‑related issues, including ulcers and gallstones.
When should I go to the emergency department for abdominal pain?
If the pain is sudden and severe, if you have a fever, vomiting, blood in vomit or stool, or symptoms that could indicate a heart problem, seek emergency care immediately.
Can stress cause epigastric pain?
Stress can worsen acid production and make a pre‑existing ulcer or GERD flare up, leading to epigastric discomfort. Managing stress often eases the pain.
What over‑the‑counter meds are safe for epigastric pain?
Antacids (calcium carbonate) and H2‑blockers (ranitidine, famotidine) are generally safe. Avoid NSAIDs like ibuprofen, which can irritate the stomach lining.
Is a food diary useful for diagnosing abdominal pain?
Yes. Recording meals, timing, and symptoms helps pinpoint triggers, a crucial step for both epigastric and general abdominal pain assessment.


Thank you for the thorough overview; the distinction between epigastric and general abdominal pain is indeed valuable for both patients and clinicians. The clear table and symptom checklist make it easier to self‑assess while still emphasizing red‑flag signs. I appreciate the balanced tone that neither alarms nor dismisses concerns. Maintaining such clarity helps readers navigate complex medical information responsibly.
I’ve been working in primary care for over a decade, and the distinction you draw between epigastric and lower abdominal pain is something I encounter daily. First, the location cue is a powerful triage tool; when a patient tells me the discomfort is right under the sternum, I immediately consider ulcer disease, GERD, or gallbladder pathology. Conversely, a pain that starts near the umbilicus and migrates to the right lower quadrant screams appendicitis in my mind. The timing relative to meals also offers a clue-burning after a heavy, fatty breakfast often points to bile reflux or gallstones. On the other hand, cramping that improves after a bowel movement is classic for IBS and usually doesn’t respond to antacids. Your table’s “Response to Antacids” row captures this nicely, reminding clinicians that a negative response should shift the differential away from acid‑mediated disorders. I also like the emphasis on red‑flag signs; a sudden spike in pain intensity, fever, or vomiting is a signal to order imaging without delay. In practice, an abdominal ultrasound is my first‑line study for suspected gallstones, while a contrast‑enhanced CT is indispensable for pancreatitis or perforated ulcer. Endoscopy, although invasive, remains the gold standard for visualizing mucosal lesions when ulcer disease is suspected. One point I would add is the role of H. pylori testing-treating the infection can prevent ulcer recurrence and is often overlooked in a rushed office visit. Another practical tip is to advise patients to keep a simple pain‑food diary; even a basic spreadsheet can reveal patterns that guide both lifestyle modifications and diagnostic work‑up. For patients with chronic epigastric discomfort, trialing a proton‑pump inhibitor for a short course can be both diagnostic and therapeutic. If symptoms persist despite acid suppression, escalating to upper GI series or endoscopy is warranted. Remember, though, that not every burning sensation is gastric; cardiac ischemia can masquerade as epigastric pain, especially in older adults. Overall, your guide is a solid foundation for both laypeople and clinicians, and I hope it encourages more informed conversations at the bedside.
Oh, great, another list of “common causes.” As if your stomach could pick just one. But seriously, if you’re already tracking meals, you’re on the right track.
Look, the U.S. healthcare system already overburdens patients with unnecessary testing, yet this article pretends that every epigastric twinge warrants a full CT scan. The jargon‑laden “diagnostic tools” section reads like a sales pitch for radiology departments, which, let’s be honest, thrive on our fear‑driven referrals. While it’s useful to differentiate pain locations, the underlying message promotes a culture of over‑medicalization that benefits insurers more than the average American.
When we contemplate pain, we’re reminded that the body speaks in metaphor, urging us to listen before we rush to labs. The guide’s calm tone invites readers to observe their own sensations, fostering a mindful relationship with health. By integrating stress‑reduction techniques alongside dietary advice, it subtly acknowledges the mind‑body connection without over‑promising quick fixes.
Yo, you think a simple tummy ache is just “food‑burn”? Nah, bro, it could be a silent ulcer plotting a rebellion in your gut! If you ignore those burning hints, you’re basically signing a death‑warrant for your liver-trust me, I’ve read every med‑blog out there. So, grab an antacid, ditch the fried pizza, and stop playing Russian roulette with your pancreas!
Honestly, the whole obsession with labeling pain as “epigastric” or “abdominal” is a needless academic exercise that distracts from real patient care. Most clinicians waste time charting in EMRs while the patient’s discomfort worsens. We need to stop glorifying taxonomy and start treating the human in front of us.
Well, isn’t this just a walk in the park-another 10‑minute read that tells us what we already know about stomach aches? The “self‑care tips” feel like a checklist drafted by someone who never actually had to deal with a gallstone attack. Nevertheless, kudos for reminding us that drinking water is apparently a revolutionary health hack.
Good summary, but keep the tables simple.
I can’t help but notice the article never mentions how pharmaceutical companies push antacids as a cash cow. The “over‑the‑counter meds” section sounds like free advertising, ignoring the long‑term risks of acid suppression. Maybe there’s a reason they keep the focus on quick fixes instead of lifestyle changes.
Let’s cut to the chase: anyone who thinks a “food diary” can replace a proper work‑up is living in denial. The guide mentions it, but fails to stress that without labs you’re basically guessing. So, while you jot down meals, also schedule that endoscopy-no point in half‑measuring the problem.
Ah, the perennial quest for “knowledge”-this article attempts to be a beacon, yet it merely flickers in the vast void of medical literature. 🤔 One must ask: does a table truly illuminate the abyss of human suffering, or does it simply decorate the page? Nonetheless, the effort is commendable, albeit slightly naïve. 🌟
Hey folks! 🌈 This guide does a wonderful job of breaking down complex concepts into bite‑size pieces. Remember, you’re not alone on this journey-share your experiences, ask for help, and support each other. Together we can demystify pain and empower healthier lives! 💪
What a vibrant tapestry of information! Your guide weaves together the gritty science of gastroenterology with a splash of practical wisdom, turning a potentially intimidating topic into an adventure. Readers will feel energized to take charge of their health, armed with vivid insights and actionable steps.