
Spinal Procedure Anticoagulation Timing Calculator
Patient & Medication Profile
Select your medication and procedure type to see the recommended safety timeline.
Imagine you are scheduled for a routine spinal procedure to manage chronic pain or support labor. You feel prepared. But there is one detail that could turn this safe, common intervention into a medical emergency: the blood-thinning medication you take daily. Spinal epidural hematoma is a rare but potentially catastrophic complication where blood accumulates in the spinal canal, compressing the nerves. While the incidence rate is low-roughly 1 in 150,000 for standard epidural blocks-the consequences of missing the warning signs or mishandling your medication timing can be life-altering, including permanent paralysis.
The intersection of modern anticoagulation therapy and neuraxial procedures creates a complex clinical puzzle. With millions of spinal procedures performed annually alongside a booming market for blood thinners, understanding how these two worlds collide is not just academic; it is a matter of patient safety. This article breaks down the real risks, the specific timing protocols recommended by leading authorities like the American Society of Regional Anesthesia and Pain Medicine (ASRA), and what you need to know to advocate for your own care.
Understanding the Risk: Why It Happens
To grasp why this risk exists, you have to look at anatomy. The spinal cord sits within a tight bony canal. When a needle is inserted for an epidural or spinal block, it pierces through tissue that contains small blood vessels. In a healthy person with normal clotting factors, any tiny bleed stops almost immediately. However, if you are on anticoagulants, your blood’s ability to clot is intentionally suppressed. If a vessel bleeds during or after the procedure, that blood has nowhere to go. It pools in the potential space between the dura mater (the protective covering of the spine) and the ligamentum flavum.
Because the spinal canal is so confined, even a small volume of blood-just 1 to 2 milliliters-can create significant pressure. This pressure compresses the spinal cord or nerve roots, cutting off oxygen supply. The result is rapid neurological deterioration. Studies show that symptoms typically develop within 12 hours of the procedure. The most common early sign is midline back pain, reported in 93% of cases. This is often followed by sensory deficits, motor weakness, and eventually bowel or bladder dysfunction.
The critical factor here is time. A pivotal study by Afshari et al. demonstrated that surgical decompression within 8 hours of symptom onset leads to complete neurological recovery in 79% of patients. Wait until 24 hours, and that recovery rate plummets to just 9%. This narrow window makes early recognition and immediate action vital.
Anticoagulant Classes and Their Specific Risks
Not all blood thinners carry the same risk profile. The type of anticoagulant, its dosage, and how long it stays active in your system determine the danger level. Let's break down the major categories.
| Anticoagulant Type | Key Risk Factor | Pre-Procedure Window | Post-Procedure Resumption |
|---|---|---|---|
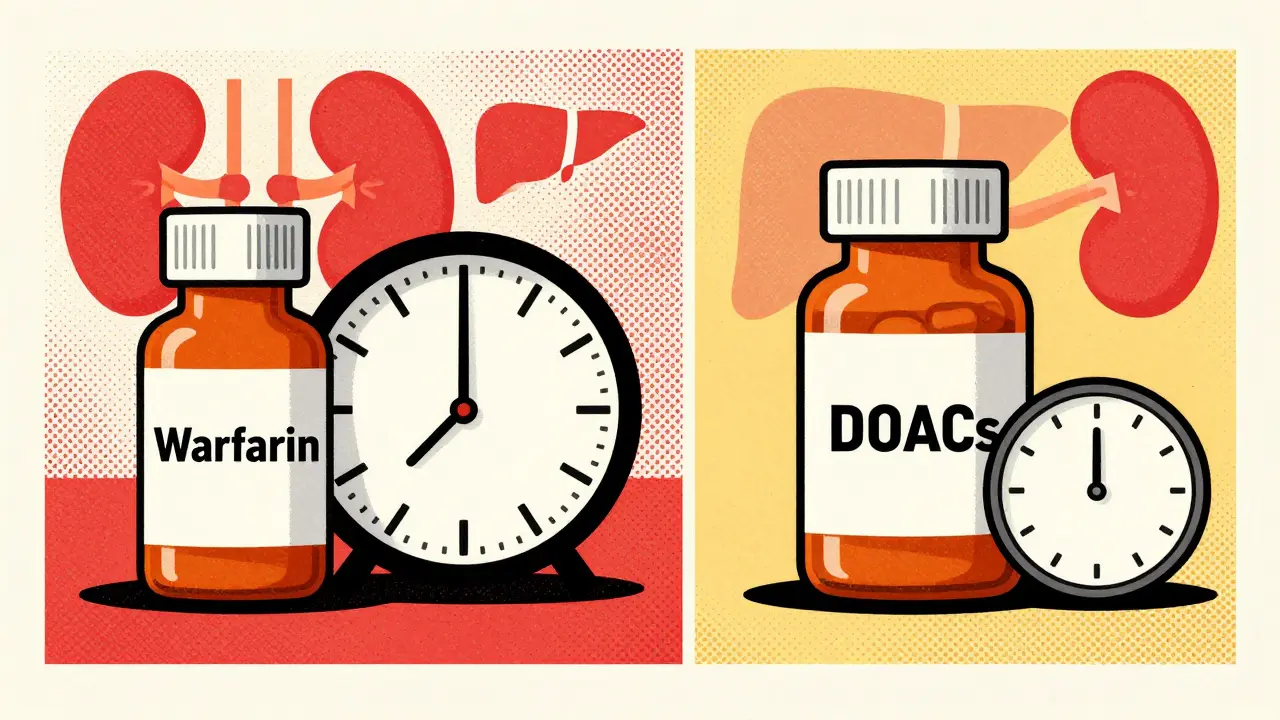
| Warfarin | INR Level | INR must be <1.4 | 4 hours (single shot) / 6 hours (catheter) |
| LMWH (e.g., Enoxaparin) | Dosing Interval | 10-12 hours (prophylactic) / 24 hours (therapeutic) | 2 hours (single shot) / 4 hours (catheter) |
| DOACs (e.g., Apixaban, Rivaroxaban) | Renal Function | 48 hours (normal renal function) | Variable based on renal clearance |
| Antiplatelets (e.g., Aspirin) | Monotherapy vs. Dual Therapy | Aspirin alone often continued; Clopidogrel stopped 7 days prior | As per surgeon/anesthesiologist discretion |
Warfarin requires careful monitoring via the International Normalized Ratio (INR). Research indicates that an INR greater than 1.4 is associated with an 8.7-fold increased risk of hematoma. Therefore, checking your INR within 24 hours before the procedure is non-negotiable. If your levels are too high, the procedure should be postponed.
Low Molecular Weight Heparin (LMWH), such as enoxaparin, presents a different challenge because it is not easily monitored with standard blood tests. The risk depends heavily on the timing of the last dose. Administering LMWH within 8 hours before a procedure increases the risk significantly compared to waiting 24 hours. Therapeutic doses (used for treating existing clots) require a longer washout period than prophylactic doses (used for prevention).
Direct Oral Anticoagulants (DOACs) like rivaroxaban and apixaban have become popular due to their predictable pharmacokinetics. However, they still pose a risk if timing is ignored. For patients with normal kidney function, a 48-hour cessation is generally recommended. For those with renal impairment (creatinine clearance below 50 mL/min), this window extends to 72 hours. Ignoring this distinction can lead to dangerous accumulation of the drug in the body.
There is ongoing debate regarding antiplatelet agents. Some experts argue that continuing aspirin poses minimal risk, citing large studies with zero complications. Others warn that dual antiplatelet therapy (combining aspirin with clopidogrel) increases risk nearly four-fold and should be avoided for at least seven days before invasive procedures. This discrepancy highlights the need for individualized assessment rather than a one-size-fits-all rule.
Identifying High-Risk Scenarios
Beyond the medication itself, several other factors compound the risk. Understanding these helps you and your healthcare team make safer decisions.
- Technical Difficulty: Multiple needle passes increase trauma to the tissue. Having three or more attempts increases the risk by over six times. A traumatic puncture, identified by blood-tinged cerebrospinal fluid, raises the risk nearly twelve-fold.
- Patient Age and Health: Advanced age (over 70 years) is an independent risk factor, increasing odds by 3.7 times. Renal impairment is particularly dangerous because many anticoagulants are cleared by the kidneys. Poor kidney function means the drug stays in your system longer, extending the bleeding risk.
- Anatomical Factors: Conditions like spinal stenosis reduce the available space in the spinal canal, making any amount of bleeding more likely to cause compression.
- Catheter Placement: Leaving an epidural catheter in place carries a higher risk than a single-shot injection. This is because the catheter can erode into a blood vessel or cause irritation over time, leading to delayed bleeding even after the initial procedure is complete.
A retrospective study of over 12,000 spinal procedures identified additional red flags: intraoperative blood loss exceeding 1 liter, hemoglobin levels below 10 g/dL, and an INR above 2.0 within 48 hours post-procedure. These metrics serve as objective markers for heightened vigilance.
Navigating Guidelines and Clinical Practice
The American Society of Regional Anesthesia and Pain Medicine (ASRA) publishes the gold-standard guidelines for managing anticoagulation around neuraxial procedures. Updated regularly, these guidelines emphasize individualized risk-benefit assessments. They do not simply say "stop all meds." Instead, they provide structured algorithms based on the specific drug, dose, and patient factors.
Despite clear guidelines, implementation errors remain a significant issue. A survey of pain management physicians revealed that only 58% could correctly identify all timing requirements for various anticoagulants. Nearly a third reported experiencing at least one "near-miss" event due to timing errors. This gap between knowledge and practice underscores the importance of clear communication between you, your primary care provider, and the anesthesia team.
Documentation plays a crucial role. The FDA found that in a significant portion of reported hematoma cases, there was inadequate documentation of the patient's anticoagulation status at the time of the procedure. Always ensure your medical records clearly list every medication, including over-the-counter supplements like fish oil or vitamin E, which can also affect clotting.

What Should Patients Do?
If you are facing a spinal procedure and take blood thinners, you are not powerless. Here is a practical checklist to protect yourself:
- Disclose Everything: Tell your anesthesiologist about every medication and supplement you take. Be specific about dosages and the time of your last dose.
- Verify Timing: Ask specifically: "Based on my current medications and kidney function, when should I stop taking them before the procedure?" Do not assume the standard rules apply to your unique health profile.
- Know the Warning Signs: After the procedure, monitor yourself closely. Severe, worsening back pain, numbness in the legs, difficulty urinating, or weakness in the limbs are red flags. Do not dismiss these as normal post-procedure soreness.
- Seek Immediate Help: If you experience any neurological symptoms, go to the emergency room immediately. Tell them you recently had a spinal procedure and are on anticoagulants. Time is muscle-and nerve.
New tools are emerging to help clinicians navigate this complexity. Mobile apps and digital checklists are becoming more common in hospitals to ensure no step is missed. Additionally, new biomarkers, such as serum GFAP levels, are being researched to detect impending hematomas earlier than traditional symptoms allow. While these technologies are promising, they are not yet universally available, making personal awareness and adherence to current guidelines the best defense.
The Bottom Line
Spinal epidural hematoma is a rare event, but its severity demands respect. The combination of anticoagulants and neuraxial procedures requires precise coordination. By understanding the specific risks associated with your medications, adhering strictly to timing protocols, and recognizing early warning signs, you can significantly mitigate these dangers. Open communication with your healthcare team is your strongest safeguard against this devastating complication.
Can I get an epidural if I am on blood thinners?
Yes, but strict timing protocols must be followed. Most patients can safely receive epidurals if their anticoagulants are paused for the appropriate duration before the procedure and resumed only after confirmed hemostasis. The specific pause time depends on the type of medication and your kidney function.
How soon after an epidural can I restart my blood thinners?
For single-shot injections, restarting is often permitted 2 to 4 hours later, provided there are no signs of bleeding. If an epidural catheter is used, it must be removed first, and anticoagulants are typically restarted 4 to 6 hours after removal. Always follow your anesthesiologist's specific instructions.
What are the first signs of a spinal hematoma?
The earliest and most common sign is severe, persistent midline back pain. This may be followed by numbness or tingling in the legs, weakness in the lower extremities, and difficulty controlling bladder or bowels. Symptoms usually appear within 12 hours of the procedure.
Is aspirin safe to continue before a spinal procedure?
Current guidelines suggest that aspirin monotherapy poses minimal risk and may be continued. However, if you are on dual antiplatelet therapy (e.g., aspirin plus clopidogrel), the second agent should typically be stopped 7 days prior. Always consult your doctor, as individual cardiovascular risk factors may change this recommendation.
Does kidney disease affect the safety of spinal procedures on anticoagulants?
Yes, significantly. Many anticoagulants are eliminated by the kidneys. Impaired kidney function slows this process, causing the drug to remain active in your body longer. This often requires extending the pre-procedure cessation window from 48 to 72 hours or more to ensure safety.


It is fascinating how we treat the human body like a machine that can be serviced on a whim, yet we ignore the fundamental biological reality that clotting is not merely a nuisance but a vital survival mechanism. The arrogance of modern medicine assumes that because a procedure is 'routine,' it is safe, ignoring the chaotic variables of individual physiology. When you introduce anticoagulants into this equation, you are essentially playing Russian roulette with your spinal cord, and most patients are too passive to even check if the gun is loaded. The statistics provided here are comforting in their rarity, but they do little to assuage the existential dread of knowing that one bad needle stick could leave you permanently disabled. We have become so desensitized to medical interventions that we forget the profound vulnerability of exposing our central nervous system to such risks. It is a testament to our collective ignorance that we accept these guidelines as gospel without questioning the underlying power dynamics that prioritize convenience over caution. The real issue is not just the blood thinners, but the systemic failure to educate patients about their own bodies. We are handed pills and told to take them, then handed needles and told to sit still, all while the experts debate the nuances of INR levels in rooms we cannot enter. This article is a necessary wake-up call, albeit a bit late for those who have already suffered the consequences.
The ASRA guidelines mentioned are indeed the gold standard, but implementation is where things often fall apart. I've seen cases where the timing window was missed by just an hour due to scheduling conflicts, leading to unnecessary cancellations or worse, proceeding with elevated risk. The key takeaway for patients is to have a pre-procedure consultation specifically focused on anticoagulation management, separate from the general anesthesia consult. Don't assume the team has checked your renal function or recent labs; bring your own records and ask direct questions about the washout period for your specific medication.
This is really helpful info, especially for people like me who are on DOACs for atrial fibrillation. I always worry about stopping my meds, but the 48-hour rule makes sense when you think about how long they stay in the system. Thanks for breaking down the difference between prophylactic and therapeutic doses, that’s something I didn’t fully understand before. It gives me more confidence to talk to my doctor about the timing.
One must consider the geopolitical implications of pharmaceutical marketing influencing these 'guidelines.' The push for DOACs is not solely based on efficacy but on patent expirations and market share wars. The 48-hour cessation window is a convenient fiction that allows hospitals to maintain throughput while shifting liability onto the patient's non-compliance. Furthermore, the definition of 'renal impairment' is often manipulated to include borderline cases, thereby extending the exclusion criteria and reducing the pool of eligible candidates for neuraxial anesthesia. This creates a self-fulfilling prophecy where complications are rare because the high-risk patients are systematically excluded or misdiagnosed. The data presented here is likely cherry-picked from controlled trials that do not reflect the chaotic reality of emergency departments.
You people are walking around blindfolded. If you don't know your exact last dose time down to the minute, you shouldn't be getting any procedure. It’s negligence plain and simple. Stop blaming the doctors and start taking responsibility for your own stupidity. If you’re on blood thinners, you are a ticking time bomb, and most of you are too lazy to track your intake properly. Wake up!
I totally get the anxiety around this, especially with the kidney stuff. My mom had issues with her creatinine levels affecting how long her meds stayed active, so we had to wait way longer than usual. It was stressful but the anesthesiologist was super chill and explained everything step by step. Just make sure you write down every med and supplement, even the weird ones like fish oil, cause they do matter. Hope everyone stays safe out there!
ugh. another scary medical post. i hate reading this stuff because it just makes me paranoid. why can't doctors just be careful? 😒
The notion that a 48 hour window is sufficient for all DOACs is a gross oversimplification that ignores the nuanced pharmacokinetics involved. In reality, the half life varies significantly based on age weight and genetic polymorphisms in CYP enzymes which are rarely tested in clinical practice. Most practitioners operate under a veil of ignorance assuming that standard protocols apply universally which is a dangerous assumption. The fact that we rely on such crude metrics as creatinine clearance rather than actual drug levels is indicative of a healthcare system that values efficiency over precision. It is absurd that we continue to use these blunt instruments when technology exists to measure coagulation status directly. The average practitioner is woefully unprepared to handle the complexities of modern anticoagulation therapy and continues to prescribe it with reckless abandon.
Let us delve deeper into the pharmacological mechanisms at play here. The interaction between LMWH and antithrombin III is not linear, and the bioavailability can be affected by subcutaneous tissue perfusion, which is often compromised in elderly patients or those with edema. This means that the standard dosing intervals may not accurately reflect the peak anticoagulant effect in all individuals. We must advocate for a more personalized approach, potentially utilizing anti-Xa assays to guide timing decisions in high-risk scenarios. This would provide a more objective measure of residual anticoagulant activity than relying solely on elapsed time since the last dose.
The entire premise of this article is flawed because it assumes that the risk of hematoma is the primary concern. In reality, the risk of thromboembolic events from stopping anticoagulation far outweighs the risk of a spinal hematoma in most patients. By focusing so heavily on the bleeding risk, we are inadvertently encouraging unsafe discontinuation of vital medications. The guidelines are biased towards avoiding litigation from rare catastrophic events rather than optimizing overall patient outcomes. Most patients will never develop a hematoma, but many will suffer strokes or DVTs if their anticoagulation is interrupted unnecessarily. The narrative needs to shift towards balancing these risks rather than fear-mongering about bleeding.
I think it’s important to remember that behind every statistic is a person trying to navigate a complex system. Whether you are a patient or a provider, communication is key. There is no judgment here, just a need for clarity and support. If you have concerns, speak up. Your health is your journey, and having open conversations with your care team can make all the difference. Let’s create a space where questions are welcomed and fears are addressed with empathy and knowledge.
In my culture, we often rely on traditional remedies alongside prescribed medications, which can complicate these timelines. For instance, certain herbal supplements like turmeric or ginkgo biloba are commonly used and can affect clotting. It’s crucial for healthcare providers to be culturally competent and ask about these practices openly. Ignoring them can lead to unexpected bleeding risks. We need to bridge the gap between Western medical protocols and diverse health beliefs to ensure safety for everyone.